Application of Geospatial Data to Major Public Health Emergency Response??A Simulation Study
for 2020 COVID-19 Epidemic Management
Li, J. Z.1,3 Xiao, X.2,9 Zhao, B. Y.2,9 Xie, X.2,3 Wei, Y.4 Cheng, Y. Q.5
Su, F.6 Zhang, Z. L.7
Wang, Y. X.8 Xue, B2,3*
1. College of Urban and Environment Sciences,
Xuchang University, Xuchang 461000, China;
2. Institute of Applied Ecology, Chinese Academy
of Sciences, Shenyang 110016, China;
3. Key Lab for Environmental Computation and
Sustainability of Liaoning Province, Shenyang 110016, China;
4. School of Geographical Sciences, Northeast
Normal University, Changchun 130024, China;
5. College of Geography and Environment Science,
Hainan Normal University, Haikou 571158, China;
6. School of Economics & Management, Shaanxi
University of Science & Technology, Xi??an 710021, China;
7. College of Earth and Environmental Sciences,
Lanzhou University, Lanzhou 730000, China;
8. Scientific Research Center of Gansu Province
Maternity and Child-care Hospital, Lanzhou 730030, China;
9. University of Chinese Academy of Sciences, Beijing 100049, China
Abstract: The numbers of
infected people and the planning of emergency medical facilities are the key
factors for the response of major public health emergency. The conclusions are as follows: (1) The number of potential
infections in Wuhan city based on migration index is close to the actual data,
which indicates that migration data is of great significance for supporting
public health emergency response; (2) Based on geospatial location technology,
emergency medical facilities can be identified quickly, which provides scientific
support for the layout of medical staffs?? resting places and other supporting
logistics. Given the fact that the application of geosciences in major public health
events are relatively weak, this study proposes that in the future, we should
further explore the establishment of medical geosciences data sharing
mechanism, reserve emergency technical capabilities, and make real contribution
to the national comprehensive emergency management.
Keywords: COVID-19
epidemic; medical
geography; geoscience
big data; human-land
relationship
1
Introduction
Since December
2019, COVID-19 has spread across China. On January 23, 2020, major public
health emergency level 1 response has been launched in most provinces of China.
COVID-19 has become a major public health emergency with the fastest transmission
speed, the widest infection range, and the greatest difficulty in response in
China since 1949[1]. In the emergency response of major infectious
diseases, the number of infected people is the basis for the planning and
arrangement of medical resources[2],
while the pre-arranged planning of emergency medical facilities is the core
measure for effective response[3]. For example, in the process of
the COVID-19 outbreak, infected people were delayed in treatment or caused
secondary infection due to the shortage of medical resources and lack of
isolation beds, which, to some extent, aggravated the epidemic[4].
At the same time, due to the inadequate monitoring or early problems such as
insufficient understanding, the exact number of infected people in Wuhan or
Hubei has been in a state of ??black box[5]??, which makes the emergency medical
facilities either under-supplied or over-supplied due to lack of timely and
accurate information.
The
spatial-temporal nature of public
health emergency events (the mobility of the infected objects) and the
following response (the resources demand and supply) make it have the common
nature of geography study[6]. In
a major outbreak period, the organization of efficient emergency dispatch
involves a lot of spatial and attribute information[7].
The efficient
processing, extraction, analysis, and sharing of these information cannot be
separated from the integrated use of geographic information technology[8].
For example, during the SARS period in 2003, the Institute of Geographic
Sciences and Natural Resources Research, Chinese Academy of Sciences applied the geostatistical analysis
technology to develop the ??National
SARS epidemic control and early-alarm geographic information system?? for the
collection, management, analysis, prevention, and control measures of SARS
epidemic information[9]. Therefore, it is essential to carry out the
study of the epidemic from the perspective of geoscience and explore the
technology to accumulate experience and technology in epidemic emergency
management, to improve
the supporting capacity of geography in the decision-making[10].
A
review of the development of COVID-19, especially the epidemic response in Wuhan,
shows that there are two key problems, the prediction of the number of infected
people, and the allocation of emergency medical facilities. Although some studies have predicted of infected objects[11?C12],
they were mainly based on the epidemiology or public health method, and the
prediction results are prone to errors because these models were based on low
reliable notification data. On the other hand, emergency medical facilities allocation,
especially the requisition of isolation points, invited some public criticism
due to insufficient consideration of resource constrains[13].
This study developed a model to predict the
number of infected objects based on migration index, and established a multi-source
data location-selecting procedure to support the allocation of medical
resources and facilities.
2 Background
and Methods
In terms of the infected subjects prediction, we assume
that the early statistics about infected within Wuhan (Hubei), the epicenter of
the epidemic, were not good enough to support decision-making, but the statistical
data of the infected outside Hubei province were more trustworthy. The
rationale under this assumption was that the outbreak of the epidemic in Wuhan
in early period made many works out of order, including comprehensive epidemic
data collection. By contrast, most of the infected objects outside Hubei were
imported and controllable, which made the statistical data more reliable and
timely.
Under this hypothesis, we used the Baidu migration scale index and
population estimaion data of Wuhan to estimate the number of people who
returned from Wuhan in each city. Based on the official reporting of people
diagnosed with COVID-19, we estimated the infection rate of the population
flowing out of Wuhan. Finally, the potential number of COVID-19 infections in
Wuhan was estimated based on the proportion of the migrating population and the
population of Wuhan.
Selection of emergency medical resource facilities, especially the
temporary isolation point, temporary medical
facilities such as shelter, hospitals, was based on relevant standard (the
principle of prevention and treatment of infectious diseases hospital location)
and a set of spatial data, including: residential
community, infrastructure, general
hospitals, roads, and building locations. Selection of hotels was based
on the accommodation and distance to working hospital.
|
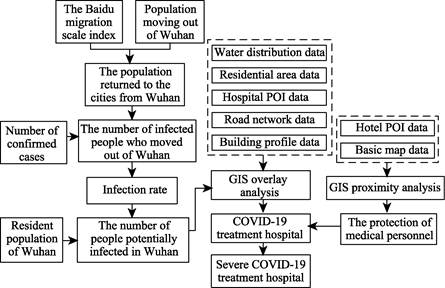
Figure
1 Flow
chart of system development
|
This spatial planning process can provide scientific reference for the estimation
of potentially infected people in Wuhan, the determination of designated
hospitals for epidemic response, and the determination of medical staffs??
resting places. The research idea is shown in Figure 1.
Wuhan POI (Point of Interest) data was collected
from Baidu map, and 670,000 pieces of POI data were collected. According to the
industry classification standard of POI data on Baidu map, hotel POI data and
general hospital POI data were cleaned and separated, and invalid data were removed. Finally, 10,731 pieces of hotel POI data
and 244 pieces of general hospital POI data were included. Baidu migration scale index was derived from Baidu migration platform
(http://qianxi.baidu.com). Through the comparing
the changes of users?? location, the number of users whose smart terminal
location has changed within 8 hours is counted.
The number of users that have changed their location was
used to represent the number of the population moving between provinces or
cities. The population scale of Wuhan city from January 10 to January 24 was
selected as the basis for calculating the outflow population before the
implementation of Wuhan lockdown. The road network data comes from Baidu map
data platform, mainly including the traffic network that can ensure the smooth
traffic flow of vehicles, such as expressway, urban expressway, national road,
provincial road, county road, and nine level road in
Wuhan. The statistics of COVID-19 infections were based on data released by
National Health Commission of China. Other auxiliary data including Wuhan building
outline data, Wuhan water area distribution data, residential district
distribution data, and administrative division data were derived from Baidu map
data platform.
3 Results and Analysis
3.1
Estimation of the Number of Potential Infections in Wuhan
According to the
implementation time of urban management and control measures in Wuhan (January 23) and the peak time of the increasing
number of daily confirmed cases in the whole country outside Hubei province
(February 3), the top 100 migration proportion by Baidu from January 10 to 24
was selected for correlation analysis with the cumulative number of confirmed
cases in corresponding cities on February 3. We found that the correlation
coefficient was 0.935, R2
was 0.874, and the sig was significantly associated with a value of 0.000.
|
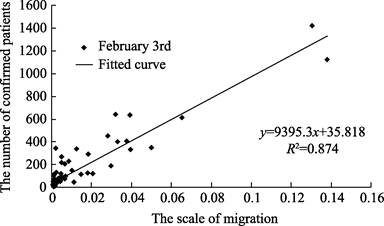
Figure 2
Relation between the number of confirmed patients and the scale of migration
|
Based on the official base number of 5
million migrant population in Wuhan, the top 100 cities
of Baidu??s migration ratio during the period from January 10 to February 3 were
calculated. These 100 cities received 4.582 million returnees from Wuhan.
According to the number of people who moved to each city and the number of confirmed
cases in each city, the ratio of the two was calculated between 0.08% and
3.53%, with an average of 0.51%, indicating that the average infection rate of
the people who moved out of Wuhan was 0.51%. Based on the average infection
rate and the resident population of 9,083,500 in Wuhan, the COVID-19 infected
population in Wuhan was estimated to be 46,000. As of February 25, Wuhan has
prepared a total of 21,962 medical beds, plus newly added 2,416 beds in
Raytheon and Vulcan Mountain field hospital[14].
There were only 24,378 medical beds available. Since our estimated infected
number was 46,000, Wuhan urgently needs to expand medical resources and
prevent secondary infection.
3.2 Site Selection for Emergency Treatment Hospital
3.2.1 Constrains
of Site Selection
According to the national standard for infectious disease hospital
construction, the sites of infectious disease hospital should avoid densely
populated areas; have convenient transportation; regular and flat terrain,
stable geological structure; have safe distance from water, harmful gas
production and storage sites, food and feed processing enterprises[15].
In order to quickly treat the infected people and make full use of the existing
general hospitals and large indoor buildings, the analysis of the location of
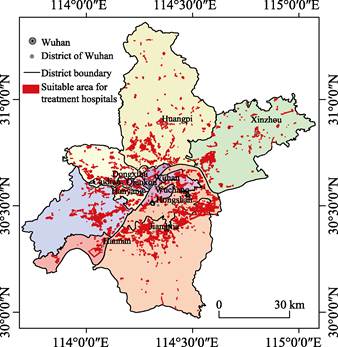
emergency hospital and temporary isolation points should be carried out. Our
spatial analysis integrated POI data, residential, population density, water
and road data to determine the area that meet the need for isolation and treatment
of infectious disease. Specifically, the site selection for hospital required:
200 m away from residential area, 500 m within major traffic, and 500 m away
from water area. According to the population distribution density of Wuhan
city, Tyson polygon law was used to define the receiving area of emergency
treatment hospitals and temporary isolation treatment points. For areas lacking
emergency treatment hospitals and temporary isolation points, field cabin
hospitals should be prioritized for consideration (Figure 3).
3.2.2
Result of Hospital Site Selection
Compared with the
spatial distribution map of 244 general hospitals in Wuhan, the general
hospitals that meet the requirements are determined. In order to reduce the
secondary potential infection of emergency treatment hospitals through sewer
and aerosol diffusion mode, especially the small scale of a high-rise building
is not conducive to more than 100 m from the pollutant dispersion intensifying
virus[16], more than 100 m tall buildings around to meet the
conditions of hospital overlay analysis, combining with the high-rise building
in Wuhan space distribution of worldwide for contingency hospitals around 200 m
more than 4,100 m high building of the hospital should be ruled out.
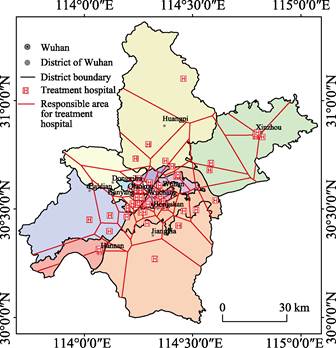
Following the aforementioned
rules, 58 hospitals were determined (Figure 4), accounting for 23.78% of the
general hospital in Wuhan. With about 13,000 of medical beds, this hospital
can??t meet the needs of the isolation and treatment of potential infected
patient. Therefore, in the future, emergency treatment centers should be added
in large warehouses and gymnasiums, or field hospitals should be set up in
large open parking lots and gymnasiums in qualified areas.
|
|
|
|
Figure 3 Distribution of qualified areas for emergency
response hospital in Wuhan
|
Figure 4 Distribution of potential hospitals for
emergency response in Wuhan
|
3.2.3
Evaluation of Hospital Site Selection
A comparison of
the simulated hospitals and the actual hospitals was conducted to evaluate the
rationality of the site selection method for emergency response hospitals. 20
designated hospitals and 16 square hospitals were within the qualified areas, accounting
for 41.67% of designated hospitals for emergency response. The fact that some
designated hospitals were located outside the qualified areas indicated our
model using unified criteria could be refined to accommodate the actual need in
reality. For instance in the early period, some hospitals with suitable
facility but smaller scale were also designated for epidemic response to meet
the urgent needs of a large number of infected patients. In the future, with
the advance of social and technological capacities, more factors should be
considered.
3.3 Site Selection for Supporting Facilities (Hotels)
Medical staff are the key players for the epidemic response.
Providing sufficient logistic for medical workers is the basis for their recovery[17]. Based on the
neighborhood analysis of the determined emergency treatment hospital and hotel
POI data, the hotels within the 500 m buffer zoom of the response hospitals
were chosen as the supporting facilities for medical staff. It was found that there were 902 qualified hotels (Figure 5),
accounting for 8.41% of the hotel in the city.
Due to lack of data from Wuhan cycling report, jointly
edited by Wuhan Transportation Development Strategy Institute and Meituan-Mobai
for proxy. The cycling data suggested that the main ridesharing were around
hospitals. From January 24 to March 12, a total of 43,000 person-times of
medical-related staff have been served, with an average distance of 1.42 km, indicating
that the medical staff often chose hotels close to their hospitals.
|

Figure
5 Spatial distribution of qualified emergency
service hotel in Wuhan
|
4 Discussion and Conclusion
In the course of
major public health events, due to the shortage of medical resources, some
patients were not timely treated and often become the source of secondary transmission.
The development of COVID-19 in Wuhan and the medical crisis fully reflect the
necessity of layered and graded public health response system within different
management units. Based on the relevant national standard and spatial data
analysis, the following conclusions can be summarized:
(1) A migration index based model showed that the number of
potential infections in Wuhan is close to the actual statistical data. The
migration index has the advantages of high efficiency, low cost, and fine
granularity. However, due to the biased sample size of Baidu migration data,
there were potential errors in the prediction. If mobile phone signaling data
could be combined with index of Baidu, it will greatly improve the accuracy of
the modeling.
(2) The appropriate areas for emergency medical facilities
were identified using geospatial technology and various data, including basic
geographic data such as water and traffic; residential extracted from POI data;
and social statistics like population density data. The simulated hospital
sites were in good agreement with the actual hospitals designated for emergency
response (100% for square hospitals, 41.67% for designated hospitals)/
(3) The appropriate hotels for emergency medical workers were
selected to ensure these hotels were in the 500 m buffer zone of their working
hospitals. This enabled exhausted medical works to have more time to recover
and provide better service.
It is worth noting that, the application
of geosciences to emergency response of major public health events are still in
its inception. One of the reasons is that it is still difficult to share
spatial data of medical cases. In the future, we should promote and establish
medical spatial data sharing mechanism. At the same time, we call on
geoscientists, especially those in the fields of space economy, geography and
space planning, to accumulate emergency data and technologies in their daily
research and be well prepared to make more contributions to the future
emergency response.
References
[1]
Xi, J. P.
Speech at the deployment meeting on COVID-19 epidemic prevention and control
and economic and social development [N]. People??s
Daily, 2020-02-24 (2).
[2]
Jia, J.
Study on the location of emergency medical facilities for public health
emergencies [D]. Beijing: Beijing
Jiaotong University, 2007.
[3]
Ding, S.
G., Zong, H. J., Zhang, S. X. Some thoughts on the
siting of infectious disease hospital [J]. Hospital Management Forum,
2003, 11: 63-64.
[4]
New Land
Planner. Urban new virus epidemic prevention, planning architect can do what?
[EB/OL]. https:// www.sohu.com /a/ 370635795_275005.2020-02-04/2020-03-1.
[5]
Cao, Z. D., Zhang, Q. P., Lu, X. Incorporating the human movement data
to improve epidemiological estimates for 2019-nCov [OL].
https://www.medrxiv.org/content/10.1101/2020.02.07.20021071v1, 2020-02-09/ 2020-02-09.
[6]
Zhou, C.
H., Pei, T., Du, Y. Y., et al. Big data
analysis on COVID-19 epidemic and suggestions on regional prevention and
control policy [J]. Bulletin of Chinese
Academy of Sciences, 2020, 35(2): 200-203.
[7]
Lin, F. M.
The applications of GIS technique in urban public emergency command system [J].
Geomatics & Spatial
Information Technology, 2009, 32(3): 31-33, 38.
[8]
Zhang, B.,
Huang, Q. Y., Zhang, S. B. Application of GIS to emergency rescue [J]. Geospatial
Information, 2007, 1: 105-107.
[9]
Chinese
Academy of Sciences. ??National SARS control and early warning of geographic
information system developed emergency?? progress [OL].
http://www.cas.cn/zt/kjzt/FDGX/cs/200305/t20030528_1710585 SHTML,
2003-05-28/2003-05-28.
[10]
Zhou, S.
Safety and health space planning and governance??talk to 2020 COVID-19 accidents
will [J/OL]. Urban planning, 2020-02-19.
https://kns-cnki-net.webvpn.las.ac.cn/kcms/detail/11.2378.TU.20200214. 1747.040.html.
[11]
Gu, C.
L., Zhu, J., Sun, Y. F., et al. The inflection
point about COVID-19 may have passed [J]. Science
Bulletin, 2020, 65: 865?C867.
[12]
Liu, Y.,
Yang, D. Y., Dong, G. P., et al. The
spatio-temporal spread characteristics of 2019 novel coronavirus pneumonia and
risk assessment based on population movement in Henan province: analysis of
1243 individual case reports [J]. Economic geography, 2020, 40(3): 24-32.
[13]
People??s Daily. University dormitory requisitioned into isolated points,
to avoid the trouble back at home that except students [OL]. https://baijiahao.baidu.com/s?
Id = 165824700360845 4125& WFR =spider&for=PC. 2020-02-11/2020-02-21.
[14]
Wuhan Municipal Health Commission. 2018 Wuhan General Hospital List [OL]. http://wjw.wuhan.gov.cn/front/web/
showDetail/2019040207173.
[15]
Construction
Standard [2016] NO. 131. Construction standard of infectious disease hospital
[S]. National Health and Family
Planning Commission of the People??s Republic of China. Beijing, 2016.
[16]
Lv, Y. X.
Scale tall buildings block the wind environment simulation analysis and
optimization strategy research [D]. Beijing: Beijing Jiaotong University, 2017.
[17]
Xinmin Evening News. National Health Commission of the People??s Republic
of China: medical staff is medical treatment to control the spread of main
force seven aspects to further strengthen the work of medical personnel
protection [OL]. https://baijiahao.baidu.com/s? Id=1658960586443322209&WFR=spider&for
= PC, 2020-02-19/2020-02-19.